May 2025 - 2
Author: Dr Dov Hersh
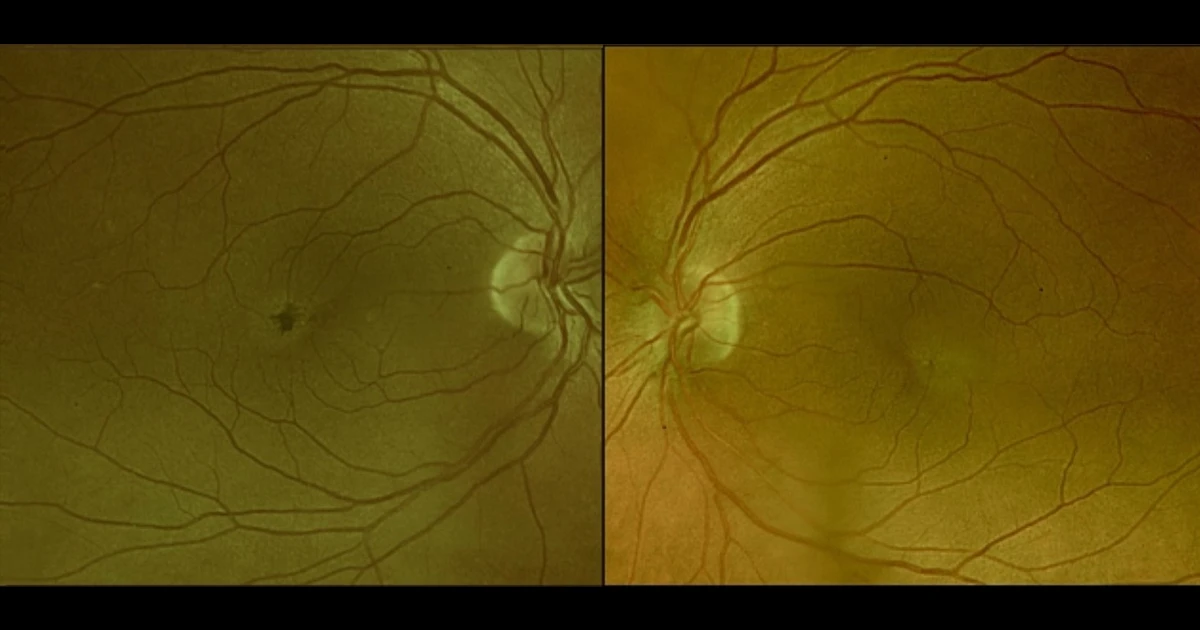
A 60-year-old caucasian male was referred with complaints of a gradual reduction in visual acuity over the last 12 months.
RVA 6/12, LVA 6/7.5. Clinical Exam of the retina displays loss of the foveal reflex, yellow crystalline spots and intra-retinal pigment hyperplasia (Figure 1 - above). OCT displays hypo-reflective inner retinal clefts, outer retinal atrophy and hyper-reflective spots (Figure 2). FFA demonstrates hyper-fluorescent capillaries temporal to the fovea (Figure 3).
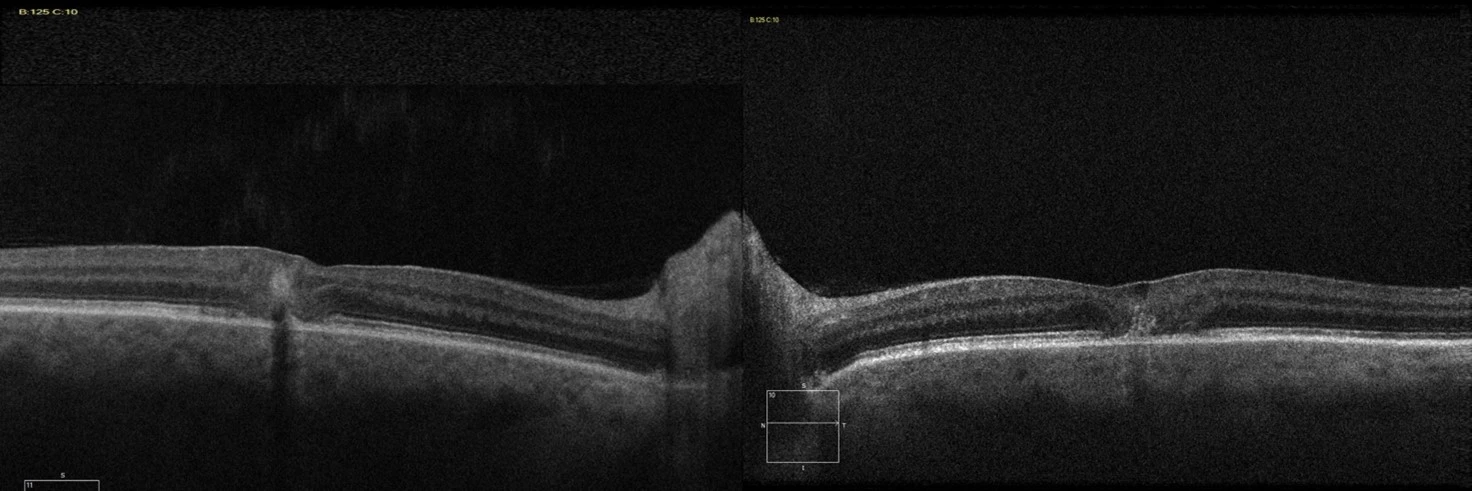
Figure 2 - OCT
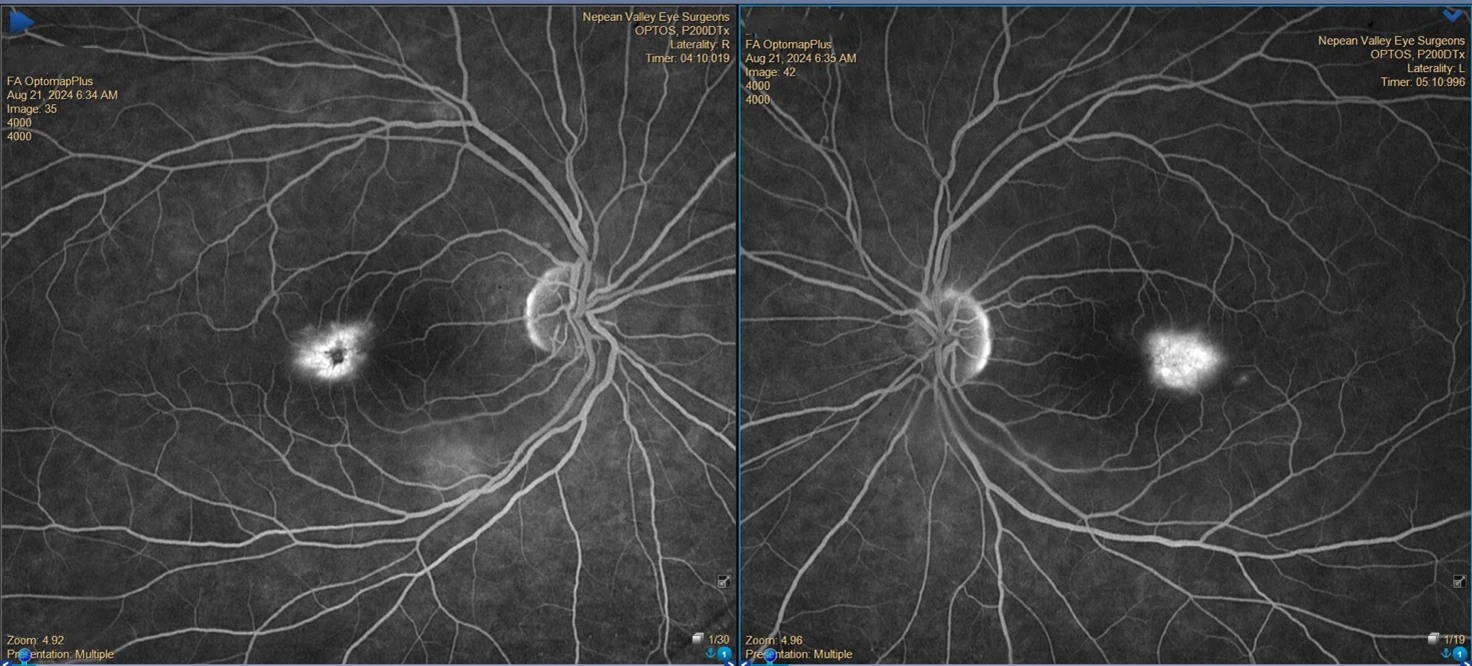
Figure 3 - FFA
What is the most valuable next step in these patient’s clinical assessment?
A - Bilateral Choroidal New Vessels
Oops! Try again
B - Previous CSR
Oops! Try again
C - Diabetic Maculopathy
Oops! Try again
D - Macular Telangiectasia
CORRECT!
Answer D
Macular Telangiectasia Type 2 (MacTel Type 2) is a relatively rare bilateral neurodegenerative condition of the macula, with an estimated prevalence of 0.01%. It typically presents in the sixth to seventh decades with symptoms such as reading difficulty and metamorphopsia. Early clinical findings are subtle and often begin in the temporal parafoveal area with signs including loss of foveal reflex, retinal greying telangiectatic capillaries and right-angled vessels. Pigment migration, crystalline deposits, and foveal atrophy occur later in the disease process. Histopathologically, there is a loss of Müller cells and photoreceptors with abnormal vessels.
OCT typically displays hypo-reflective inner retinal clefts, outer retinal atrophy and hyper-reflective spots. Early FFA shows telangiectatic capillaries temporal to the fovea with late-phase diffuse hyper fluorescence. Disease progression may result in subretinal or intraretinal neovascularization, responsive to anti-VEGF therapy, however this treatment is ineffective in non-neovascular disease, MacTel Type 2 without neovascularisation.
The first treatment targeted at MacTel Type 2 called Encelto (revakinagene taroretcel-lwey) has recently been approved by the US Food and Drug Administration (FDA). Encelto is an encapsulated cell therapy that delivers ciliary neurotrophic factor (CNTF) to the retina. This treatment aims to slow the progression of the neuronal degeneration that occurs in MacTel Type 2.