September 2025 - 1

Author: Dr John Leaney
60 yo female patient presented noticing left ptosis for the last 2 weeks. Recent history of neck manipulation whilst at the chiropractor during her routine session. She is now complaining of headache and difficulty focusing.
She has a past history of hypertension on perindopril and type 2 diabetes which is diet controlled.
Vision is 6/5 OU, IOPs 13/13. Eye movements are full but you notice a slight ptosis and anisocoria with the smallest pupil on the right side.
Pupil measurements are: R/L dark 4.5/6, light 3/3.5 with the greatest difference being in dark. Lids are 9mm/10mm.
What is the most likely cause of these findings?
A - Left third nerve palsy
Oops! Try again
B - Left Horner’s syndrome
Oops! Try again
C - Right traumatic miosis
Oops! Try again
D - Right Horner’s syndrome
CORRECT!
Answer D
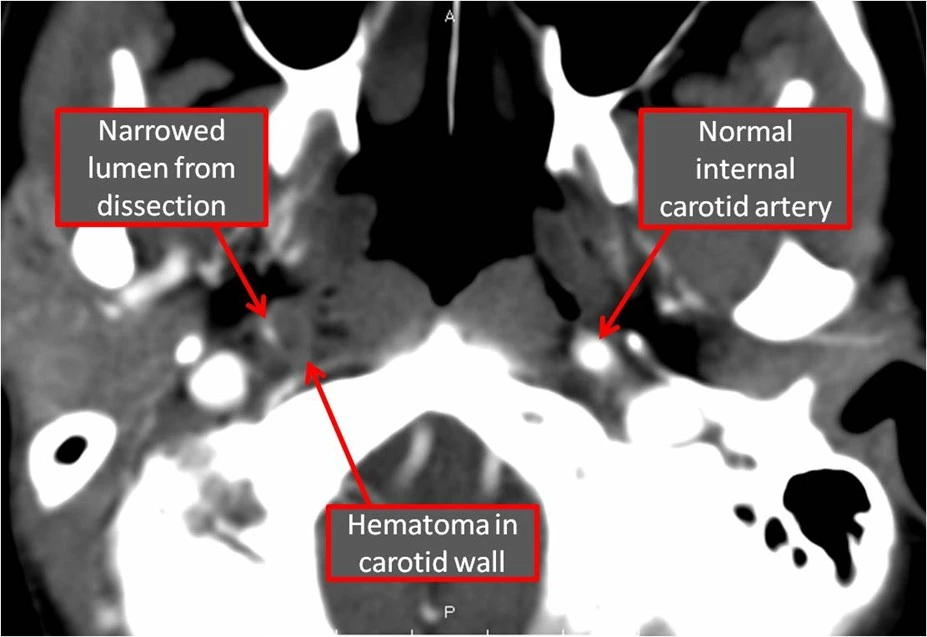
The patient has a right Horner’s syndrome post neck manipulation from a carotid dissection on the same side (traumatic Horner’s syndrome can also be seen with motor vehicle accidents, assault and post surgical). She needs urgent neuro-imaging in the form of a CT angiogram on the same day. The risk of hemispheric stroke from carotid dissection is greatest within the first 1 month. Generally aspirin is recommended to reduce the risk of stroke.
CT angiogram below showing right sided carotid dissection:
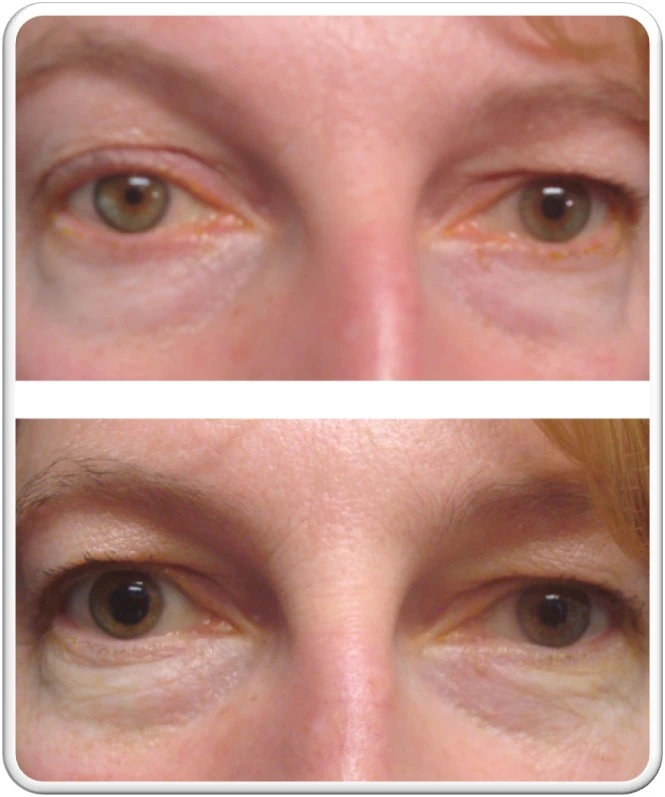
Iopidine testing of both eyes will demonstrate a reversal of ptosis and anisocoria (place 1 drop in both eyes and recheck again in 45 minutes). Note reversal of anisocoria and ptosis on the right side.
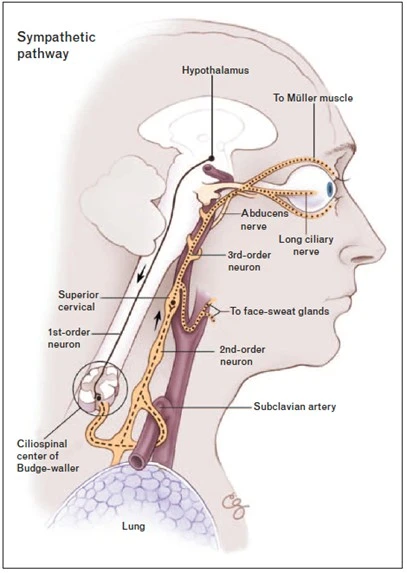
Horner’s syndrome
Triad of Horner’s – ptosis (+ reverse/low lid ptosis), miosis and anhidrosis – can be incomplete.
Horner’s syndrome is divided into 3 orders depending on the site of injury. Causes of a Horner’s syndrome depend on the level affected.
1st order – Thalamic/Hypothalamicbrainstem lesions (eg stroke, tumour, MS), Spinal cord lesions, Syringomyelia
2nd order – Lung and mediastinal tumours (classically Pancoast tumour) Children – neuroblastoma, metastases, lymphoma, jugular vein thrombosis, thyroid lesions, local trauma, iatrogenic
3rd order – ICA dissection or sclerosis, VZV, otitis media, neck trauma/inflammation, cavernous sinus pathology, headache syndrome, autoimmune autonomic ganglionopathy