February 2025 - 1
Author: Dr Brighu Swamy
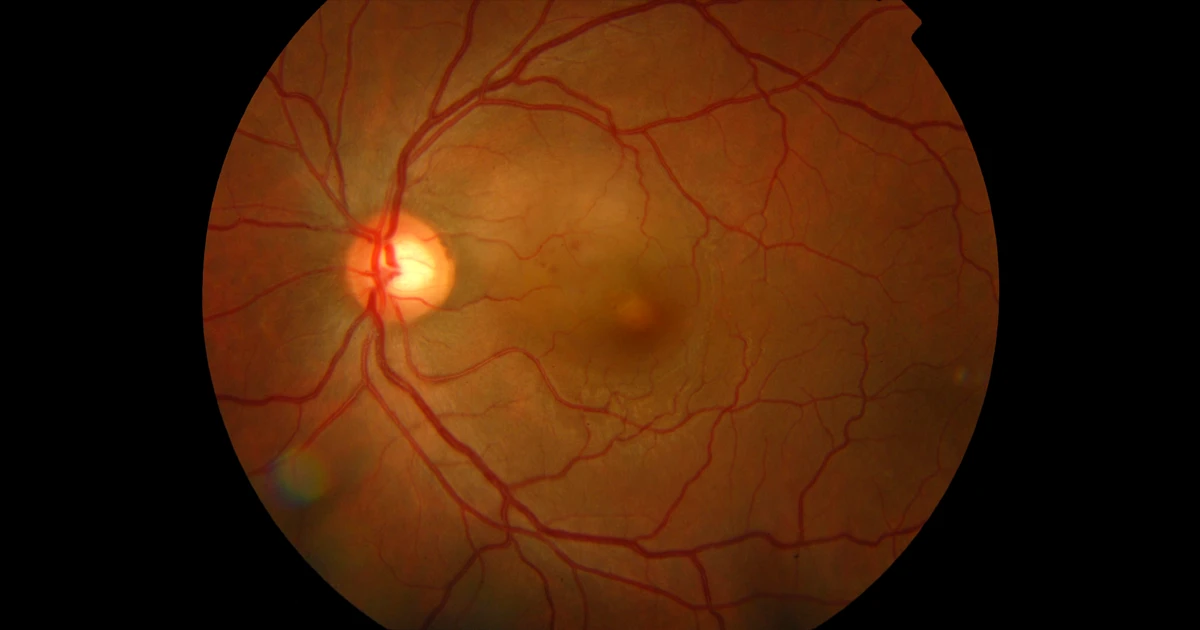
A 31-year-old male presented to our clinic after sudden loss of vision OS.
Other than this presenting complaint, he was asymptomatic, including no report of flashes, floaters, or pain. He had a recent flu-like illness and a diagnosis of hand-foot and mouth disease (HFMD).
Clinical examination revealed best corrected visual acuities of 20/20 OD and 20/48 OS. Anterior segment examination was unremarkable. Dilated examination revealed cup-to-disc ratio of 0.5 bilaterally. Retinal examination OD was unremarkable. Fundus examination OS revealed retinal pigment epithelium (RPE) mottling and subretinal fluid centrally in the macula (Figure 1 - above). Fluorescein angiography showed late staining of the lesion in the central macula (Figure 2). OCT shows neurosensory detachment and thickening of the sub RPE(Figure 3).

Figure 2

Figure 3
What is your diagnosis?
A - Central serous chorioretinopathy
Oops! Try again
B - Syphilitic Retinitis
Oops! Try again
C - Unilateral Acute Maculopathy
CORRECT!
D - Acute posterior multifocal placoid pigment epitheliopathy
Oops! Try again
Answer C
The differential diagnosis of retinal pathology leading to acute unilateral vision loss in younger patients is varied. In cases presenting with similar clinical findings to our patient, this differential may be narrowed to idiopathic choroidal neovascularization, (CSCR) acute posterior multifocal placoid pigment epitheliopathy (APMPPE), Vogt-Koyanagi-Harada syndrome, syphilitic retinitis, and unilateral acute idiopathic maculopathy.
Unilateral acute idiopathic maculopathy (UAIM) is an inflammatory entity originally described by Yannuzzi in 1991. In a case series, he describes 9 patients with abrupt onset of severe, unilateral vision loss with a flu-like prodrome. These patients shared the following characteristics:
- Sudden, severe, unilateral vision loss
- Vision loss preceded by flu-like illness
- Rapid, spontaneous, near-complete recovery of central vision
- Neurosensory macular detachment
- Characteristic macular pigment changes- residual bull’s eye maculopathy